Are you at risk of rheumatoid arthritis? Know your risk.
Dr. Sharad Jain
This article is about Rheumatoid arthritis. Know whether you are at risk of rheumatoid arthritis.
Read MoreThe Congruent-Arc Latarjet (CAL) technique allows for the reconstruction of a larger portion of the glenoid bone deficit compared to the traditional Latarjet (TL) method. This is because the inferior surface of the coracoid used in CAL is wider, offering increased bone coverage. Biomechanical studies have shown that TL provides higher initial fixation strength between the graft and the glenoid
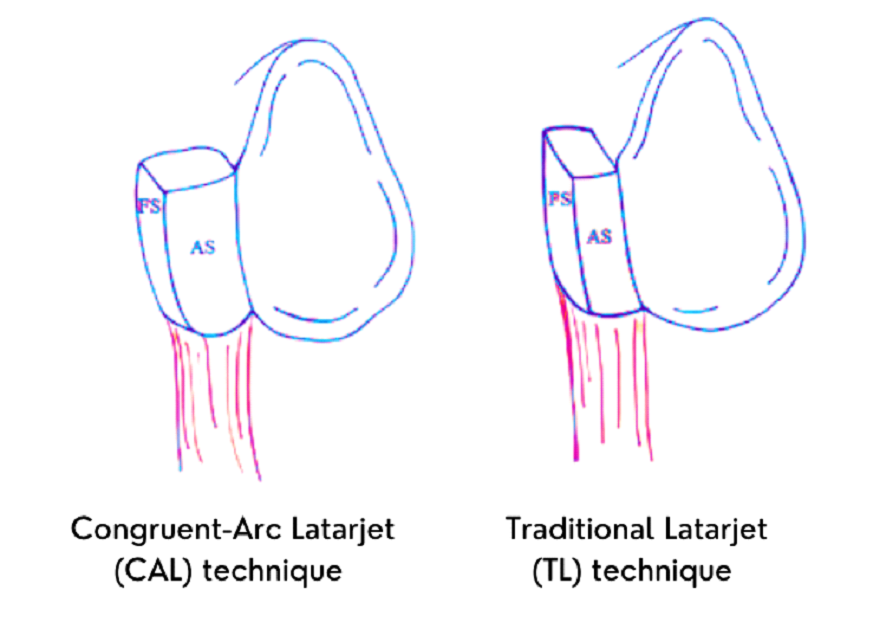
In TL, the under-surface of the coracoid remains in contact with the anterior edge of the glenoid, promoting bone consolidation through increased contact surface. However, CAL may be less tolerant of screw-positioning errors due to the shorter bone distance around the screw. Additionally, the minimal space between the CAL screw and graft wall increases the risk of screw tunnel fracture.
CAL may pose challenges for patients with small coracoids, such as small women or skeletally immature individuals. On the positive side, the CAL graft's radius of curvature is similar to the native glenoid, potentially reducing contact pressure on the glenohumeral joint and minimizing long-term degenerative changes.
The most effective surgical stabilization strategy for the unstable glenohumeral joint remains a
subject of debate. It is increasingly recognized that addressing osseous defects is crucial for biomechanical stability and good clinical outcomes, as isolated soft tissue
procedures may not suffice. The Latarjet procedure offers advantages, providing a bone block to fill anteroinferior glenoid defects and increasing the contact surface area
of the glenohumeral joint. Additionally, the repositioned conjoint tendon creates a dynamic sling effect, enhancing stability in the abduction and external rotation.
The most effective surgical stabilization strategy for the unstable glenohumeral joint remains a subject of debate. It is increasingly recognized that addressing osseous
defects is crucial for biomechanical stability and good clinical outcomes, as isolated soft tissue procedures may not suffice. The Latarjet procedure offers advantages,
providing a bone block to fill anteroinferior glenoid defects and increasing the contact surface area of the glenohumeral joint. Additionally, the repositioned conjoint
tendon creates a dynamic sling effect, enhancing stability in the abduction and external rotation.
Open and arthroscopic Bankart repairs have been the standard treatment, but arthroscopic procedures
may have higher failure rates when osseous defects are not addressed. In this study comparing the "classical" and "congruent arc" Latarjet techniques, no statistically significant
difference in force required to produce an anteroinferior shoulder dislocation was found. Both techniques appeared effective in preventing recurrent dislocations. However,
limitations of this study include its cadaveric nature and the absence of consideration for other soft tissue factors, such as capsule-labral repair or the subscapularis split.
A 5 cm skin incision is made, starting at the tip of the coracoid process and extending downward. The deltopectoral interval is located, and the cephalic vein is identified. The deltoid and
cephalic veins are retracted to the side, and a self-retaining retractor is placed between the pectoralis major and deltoid muscles to expose the conjoined tendon and coracoid.
The coracoid is divided at its base, and two holes are drilled into it. The subscapularis muscle is split in line with its fibers. A T-shaped capsulotomy is performed medially to expose
the glenoid neck. The glenoid neck is prepared by removing some tissue.
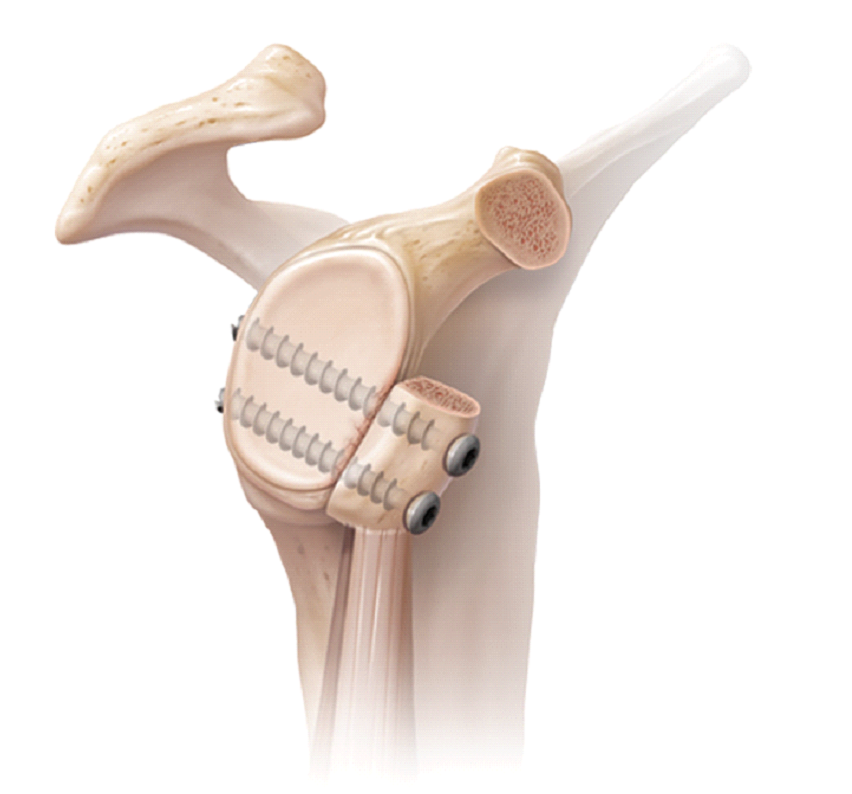
The coracoid is then fixed to the anterior glenoid rim, aligning it with the articular cartilage. This coracoid graft increases the anterior glenoid articular surface, providing added
stability to the joint. The curvature of the under-surface of the coracoid matches the glenoid surface, resulting in a congruent arc effect.
Stability is further enhanced by the overlap of the conjoined tendon with the lower half of the subscapularis muscle during abduction and external rotation.
The CAL technique in shoulder surgery is considered to be more challenging and carries a higher risk of graft fragmentation compared to the traditional Latarjet (TL) technique. This assumption is
based on the fact that the width of the bone surrounding screw fixation may decrease in the CAL method, making screw placement difficult and increasing the likelihood of graft fractures after surgery.
A study comparing the two techniques using computed tomography found that the mean bone width on each side of a 3.5-mm screw was significantly smaller in the CAL technique (4.1 ± 1.0 mm) compared to
the TL technique (7.1 ± 1.0 mm).
This study concluded that the CAL technique may be less tolerant of screw-positioning errors due to the shorter bone distance around the screw.
This finding is crucial as the Latarjet procedure is known to have a steep learning curve, requiring a significant number of procedures for surgeons to achieve proficiency.
Additionally, the CAL modification may be particularly challenging to perform in patients with very small coracoids, such as small women or skeletally immature patients.
Both the CAL and TL techniques involve screw fixation, and while some authors propose using suture buttons for graft fixation to reduce screw-related complications, there is a lack of biomechanical
studies comparing the fixation strength between the two techniques using buttons. This highlights the need for further research in this area to better understand the advantages and limitations of
each approach.
In the Indian population, the traditional Latarjet technique provides a larger surface area for a bony union of the coracoid graft compared to the congruent arc modification. The bone bridge on either
side of the 3.5-mm screws used for fixation is narrower with the congruent arc technique. This confirms that accommodating two 4 mm screws may not be feasible due to the average coracoid thickness of
7.88 mm in the Indian population. Careful consideration of fixation techniques and screw placement is vital to avoid complications and ensure successful outcomes in the Latarjet procedure for this
population.
The Latarjet procedure offers a viable option for stabilizing the unstable glenohumeral joint. The Congruent-Arc Latarjet (CAL) technique and the traditional Latarjet (TL) method each have their strengths and limitations. CAL provides a larger glenoid bone deficit reconstruction, while TL offers higher initial fixation strength. However, CAL may be more technically demanding and carry a higher risk of graft fragmentation. Consideration of patient-specific factors, such as coracoid size, is essential when choosing the appropriate technique. Continued research and clinical studies are necessary to improve surgical outcomes and provide effective treatment for patients with unstable glenohumeral joints.
We write the blogs time to time to guide website visitors about Symptoms, Causes and Treatments

Dr. Sharad Jain
This article is about Rheumatoid arthritis. Know whether you are at risk of rheumatoid arthritis.
Read More
Dr. Sharad Jain
A large number of people are effected by arthritis in Meerut. Read the article for details.
Read More